ĀÉAIRMED 2008ĀĄ
HEMS in Japan W. Nishikawa, Director
Japanese Society for Aeromedical Services
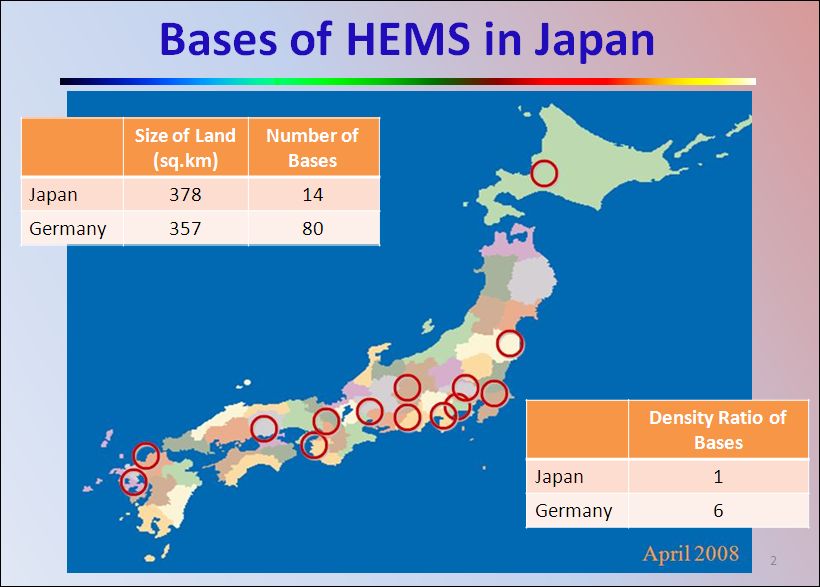
The Japanese helicopter emergency medical bases are currently located in the map shown below. We have 14 operation bases across the country. It is extremely sparse, compared with German country that has more than 80 HEMS operation bases although the land areas of Japan and Germany are almost identical. As shown in the chart, Japan's density of the base is only a one-sixth of Germany.
We call Japanese HEMS "Doctor-Helicopter" or "Doctor-Heli" in general. The helicopter to carry out HEMS service must be equipped with medical equipment for responding to an emergency case. It must be stationed in a hospital area or near hospital. The helicopter basically must be available for taking off within 3 to 5 minutes with an experienced flight doctor and a nurse onboard. Immediately after helicopter's landing on an accident site, the medical crews provide a patient with proper treatment.
It was 1999, only eight years ago, that a trial helicopter operation started, and in spring of 2001, operation of the Doctor-Helicopter system based on the trial operation results was officially inaugurated.
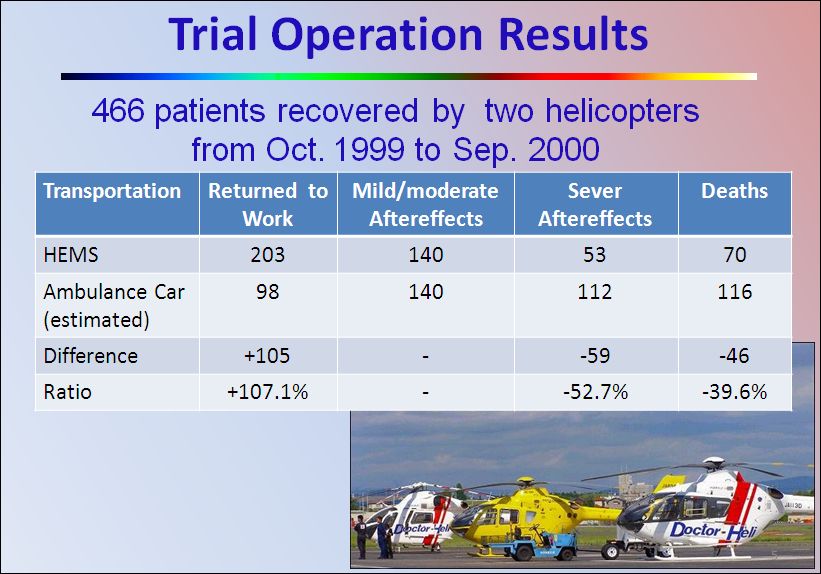
The trial operation was carried out in two different bases for one year from autumn in1999 as shown in the above chart. In the period of trial operation, number of patients that the Doctor-Helicopters responded was 466, of which the patients who died were 70. However, it is estimated that 116 patients would have died if the HEMS services were not available. In other words, lives of 46 patients were saved thanks to HEMS instead of ground ambulance. The use of HEMS could have reduced death rate by 46 percent. In addition to the reduction of death rate, 203 patients out of 466 could have returned to the working society without aftereffects. Only 98 patients presumably would have been able to return the working society if not HEMS were then available. The trial helicopter operation proved that the use of HEMS made the number of the patients who get back to works double. These facts convinced us to commence the full-fledged Doctor-Helicopter Operation from spring of 2001.
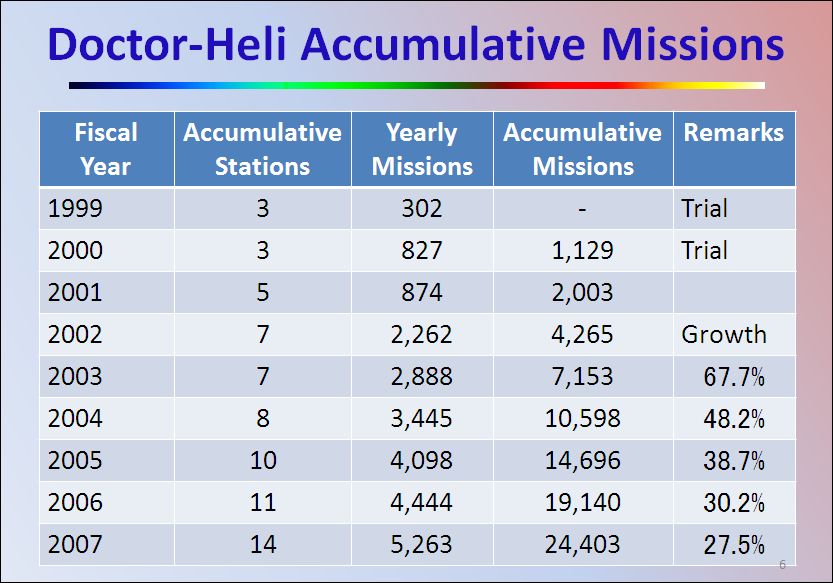
The above chart shows the accumulative missions carried out up to March 31, 2008, the end of fiscal 2007 since the inauguration of the Doctor-Helicopter system. The number of operation bases has increased to 14 and the missions totaled 24,403, as of March 31, 2008.
As shown here, number of missions achieved in fiscal 2007 was 5,263, and 4,901 patients were saved, of which 1,133 patients or 23.1 percent were the patients caused by traffic accidents. This number may seem slightly lower than the figures in Europe and the U.S.
The traffic-concerned authority has set strict regulations narrowing helicopter's landing opportunity from the reason that even opposite two traffic lanes must be closed for ensuring safety landing because the traffic lane in Japan is narrow. When deregulation is developed to ease helicopter landing, number of death in the traffic accident will decrease.
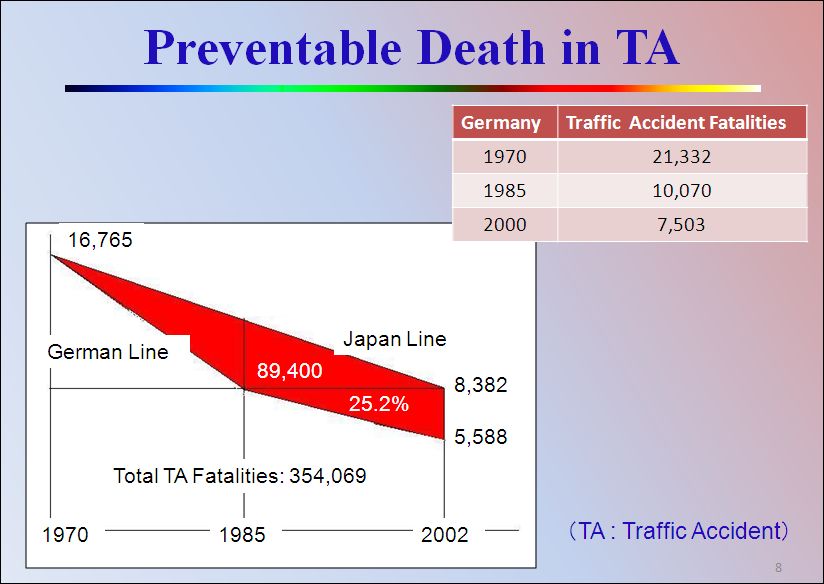
The above is to apply an example how the number of traffic fatalities was reduced to a half in Germany to the situation in Japan. A traffic fatality reached a peak of 21,332 in 1970 in Germany. It was indeed coincidentally, traffic fatality in Japan also reached a peak of 16,765 in the same year.
As you are aware, the traffic fatality in Germany was reduced to a half in the 15th year after the HEMS started, and reduced to a one-third in the 30th year. However in Japan, it took 32 years that the number of traffic fatality is reduced to a half. And so, the fatalities of Japan would have gone down like in the case of Germany if Doctor-Helicopter operation started in 1970. If this assumption is right, the area in black represents a preventable death. In other words, I dare say that the estimated fatalities of 89,400 were die to nothing or results of our poor emergency system. Its ratio is 25.2 percent.
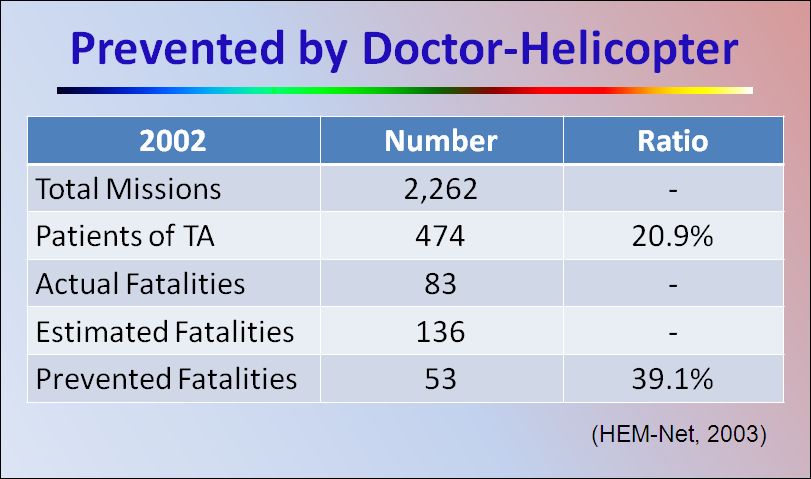
Abovementioned are my estimate based on a supposition. How will be reality? The HEM-Net has carried out investigation on reality of patients caused by the traffic accidents, and it was found that 474 missions out of total 2,262 missions in 2002 were for responding to traffic accidents. Traffic fatalities were 83. But estimated number of fatality in case of no HEMS was available is 136. Therefore, the number of prevented death was 53 or it is estimated that 39.1 percent of 136 lives were saved thanks to HEMS as shown in the table below.
The last theme of my speech on HEMS in Japan is the financial issue. Doctor-Helicopter system of Japan is financially sustained by the support from both central and local governments in equal share, based on a fixed annual amount of 180 million yen per operation base. But amount is not enough to cover actual cost, which is estimated to be 200 million yen. Insufficient subsidizations seem to be a barrier for spread of HEMS.
In order to improve this situation, a special law for medical emergency helicopter was legislated in June 2007. One of the objectives of the law is to bear the part of HEMS operation costs, adding to the abovementioned government subsidies, by health insurance, workers' accident compensation insurance, and financial resources from large scale enterprises or industrial organizations as well as donations from public. The law stipulates to materialize these ideas within the next 3 years.
Being motivated by this law, a number of local governments started making plan for establishing HEMS system. For your reference, we have 47 prefectures in Japan, of which 13 have 14 bases now, and 15 prefectures are planning the system at the present time.
Meanwhile, the Ministry of Health and Welfare of the central government has acquired a fund from fiscal 2008 budget to cover the costs of adding 3 HEMS operation bases, so at least 3 programs will be newly set up in fiscal 2008. Also two local governments will establish HEMS system by their own finance. We, therefore, will newly have 5 HEMS operation bases in this current fiscal year.
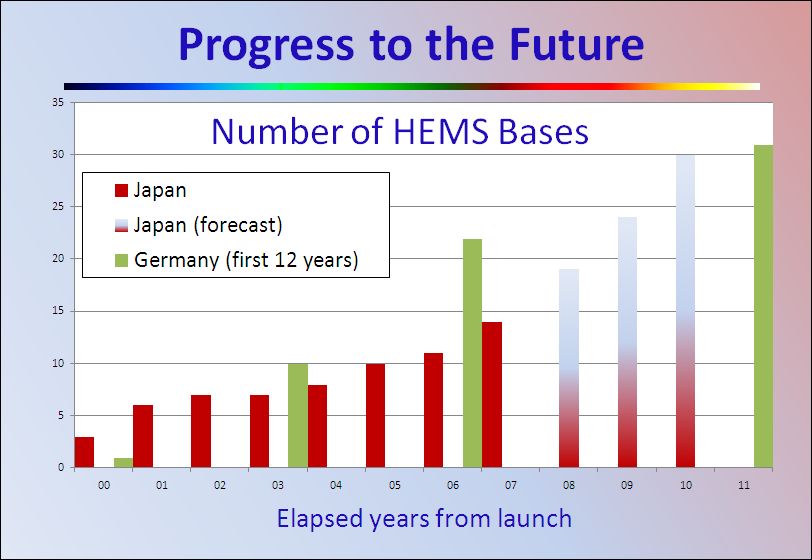
From these facts, I have an expectation that we will have Doctor-Helicopter bases as many as double within three years. It means that we have about 30 HEMS operations within 10 years from its start.
In the meantime, as shown in the above chart, the number of operation bases in Germany was 31 in 1981, the 12th year since German HEMS started. When we have 30 bases as I expect, we could nearly catch up with the state in Germany of 30 years ago.
We would also follow the past German trend to increase to 50 - 80 Doctor-Helicopter bases, and keep our effort wishing to make up Japan as a leading country in saving lives with Doctor-Helicopter system.
Finally I wish to express our deep appreciation to Mr. Gerhald Kuglar, the honourable chairman of EHAC (The European HEMS and Air Ambulance Committee) who led and supported us in many years to progress HEMS in Japan.
From left to right, Dr. Ogino, Mr. Yamano, Mr. Kuglar,
and Nishikawa after the speach at AIRMED 2008 on May 21, 2008[Related Site]
ĀiźľźžĀ@Ź¬ĀA2008.7.21Āj
Āiē\éÜā÷ĖŖāťĀj